Femoral Resurfacing with an Osteochondral Allograft for Osteochondritis Dissecans
Abstract
Osteochondritis dissecans (OCD) of the knee has multiple possible etiologies. Among these are repetitive microtrauma, disruption of normal endochondral ossification, as well genetic factors. The male to female ratio is approximately 4:1 in the United States and has been found to have the highest incidence in the African American population. Diagnosis is usually made by physical examination in association with radiographs (flexion notch view) and magnetic resonance imaging. Lesions are usually found on the lateral aspect of the medial femoral condyle. Arthroscopy continues to be the gold standard for assessing the stability of OCD lesions. Many unstable lesions may be treated with stabilization, and cartilage restoration may provide benefit; however long term data is still limited.
Case Overview
Clinical presentation
A history of the patient's knee problems should include the following questions:- Has there been any injury in the past? Any previous surgical treatment?
- What are the activities that the patient would like to return to?
- What limitations in activity, if any, have occurred as a result of the knee pain?
- Is pain or instability present at rest? Does it interfere with sleep?
- Has the patient had conservative treatments including physical therapy, rest, anti-inflammatory medication. If so, to what degree did these help?
Physical exam
Palpate the joint line for tenderness and document range of motion compared to the contralateral, normal lower extremity. Other signs and symptoms to note may include:- Aching, activity-related anterior knee pain,
- Antalgic gait,
- Effusion (only in unstable lesions)
- Mechanical symptoms (also only in unstable lesions)
Imaging
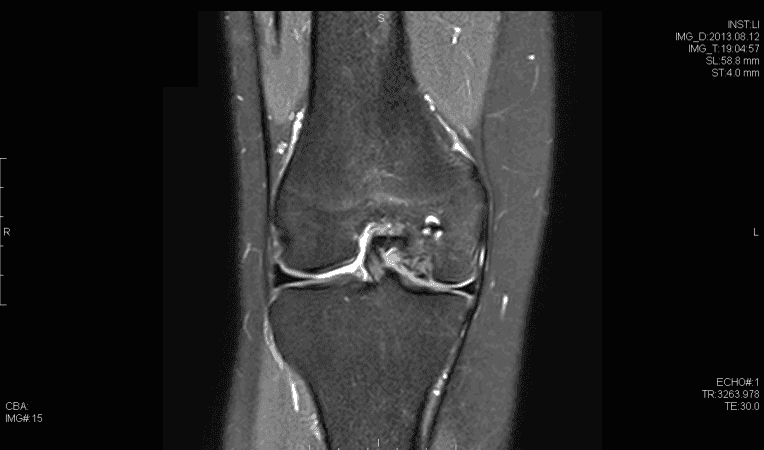
On initial assessment, obtain plain radiographs in the AP, Lateral, Tunnel and Sunrise views. In children under 7 years old, irregularities of the distal femoral epiphyseal ossification centers may mimic OCD. MRI is useful for assessing bony edema, size of the lesion and whether or not there are any loose bodies. Coronal T1 Magnetic resonance imaging demonstrating osteochondral defect
Coronal T1 Magnetic resonance imaging demonstrating osteochondral defect
 STIR Magnetic resonance imaging demonstrating osteochondral defect
STIR Magnetic resonance imaging demonstrating osteochondral defect
 Coronal T2 Magnetic resonance imaging demonstrating osteochondral defect
Coronal T2 Magnetic resonance imaging demonstrating osteochondral defect
 Sagittal T2 Magnetic resonance imaging demonstrating osteochondral defect
Sagittal T2 Magnetic resonance imaging demonstrating osteochondral defect
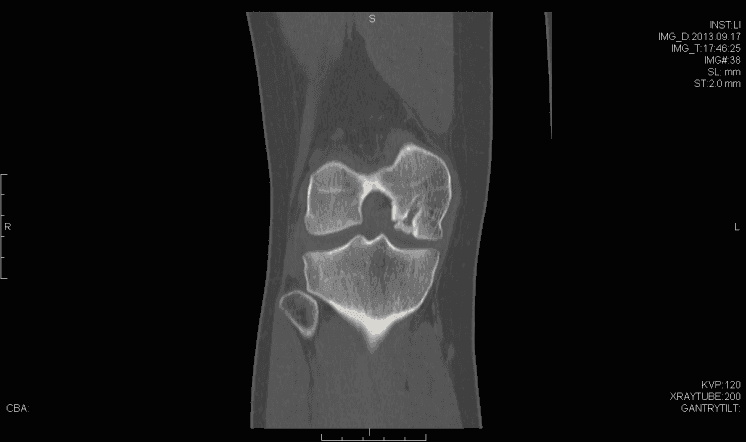 Coronal computed tomography imaging demonstrating bony aspect of the defect
Coronal computed tomography imaging demonstrating bony aspect of the defect
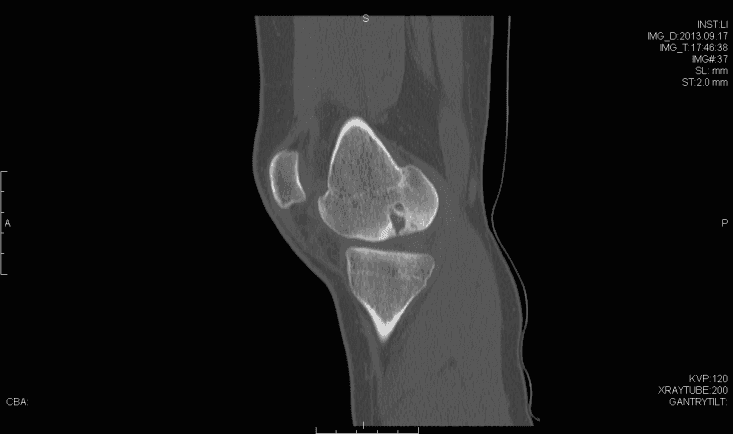 Sagittal computed tomography imaging demonstrating bony aspect of the defect
Sagittal computed tomography imaging demonstrating bony aspect of the defect
Important classification systems
International cartilage repair society (ICRS) grading- Softened area of intact cartilage
- Partial cartilage discontinuity, stable on probing
- Complete discontinuity, "dead in-situ"
- Dislocated fragment
- Small signal change, no clear margins
- OCD fragment with clear margins without fluid between fragment and bone
- Fluid partially visible between fragment and bone
- Fluid completely surrounds fragment
- Fragment displaced
Natural history
In general, smaller stable lesions with intact cartilage in skeletally immature patients are likely to heal with non-operative management2; however unstable lesions warrant arthroscopic evaluation. Overall, greater than 90% of stable OCD lesions heal with non-operative treatment measures2, while unstable lesions uniformly demonstrate deterioration if managed non-operatively.2Options for treatment
The options for treatment at this time would be a continuation of conservative treatment including physical therapy and NSAIDs; however, the patient has failed initial conservative treatment as well as prior surgical intervention. She continues to be symptomatic with pain and instability. Surgical treatment options due to the location and previous surgical intervention include osteochondral allograft, osteochondral autograft, microfracture and sandwich autologous chondrocyte implantation.Rationale for current procedure
Advantages of an osteochondral allograft technique include a shorter recovery and rehabilitation time than autologous chondrocyte implantation and less morbidity than osteochondral autografting. Microfracture may not have a role in the treatment of osteochondritits dissecans if the subchondral bone is violated.Discussion
Osteochondritis dissecans associated with stable lesions in the skeletally immature patient heals within 6 to 18 months of initiation of non-operative treatment in up to 90% of cases2, although some studies have found lower rates of healing3. OCD in the skeletally mature patient, or that associated with unstable lesions or failed conservative management, on the other hand, rarely heal without surgery2. Several techniques for managing osteochondritis dissecans lesions that have failed conservative management have been described. Kocher et. al.4 reported on trans-articular drilling of isolated stable juvenile OCD lesions (open physis) of the medial femoral condyle with intact articular cartilage surface (Stage 1-2) after 6 months of failed non-operative treatment and found radiographic healing in all patients at 4.4 months. Younger age was correlated with better outcomes. Adachi5 reviewed 12 patients with juvenile OCD that failed 6 months of non operative treatment. Retro-articular drilling was performed in 20 lesions with healing occurring in all but one patient on MRI. In the case of detached, or unstable, lesions of juvenile OCD, Kocher et al6 reported retrospectively on 26 patients. A healing rate of 85% was achieved with internal fixation with the usage of a variety of implants, and there was no significant difference between location, implant used and grade6. Others have described using autogenous osteochondral plugs that were harvested in a similar fashion as for mosaicplasty,7 with early results demonstrating healing on magnetic resonance imaging at 3 months.7 Emmerson et. al.8 used osteochondral allografting for juvenile OCD and reported 70% of patients experiencing good to excellent results at 7 years postoperatively. Finally, although micro-fracture has been described as an alternative treatment for osteochondritis dissecans, results as described by Gudas et. al.9 in a series of 50 patients with an average age of 14 years demonstrated that micro-fracture was associated with lower results and a higher failure rate when compared to osteochondral autogenous grafting.Disclosures
The author has no financial relationship with any of the companies mentioned in this article.Statement of Consent
Informed consent was obtained from the patient and all staff present in the operating room to be filmed and are aware that portions of this video will be published and freely available online.Citations
- Mubarak SJ, Carroll NC. Juvenile osteochondritis dissecans of the knee: etiology. Clin Orthop Relat Res. 1981;157:200-211. https://journals.lww.com/clinorthop/Citation/1981/06000/Juvenile_Osteochondritis_Dissecans_of_the_Knee_.33.aspx.
- Robertson WBS, Kelly BT, Green DW. Osteochondritis dissecans of the knee in children. Curr Opin Pediatr. 2003;15(1):38-44. doi:10.1097/00008480-200302000-00007.
- Wall EJ, Vourazeris J, Myer GD, et al. The healing potential of stable juvenile osteochondritis dissecans knee lesions. J Bone Joint Surg Am. 2008;90(12):2655-2664. doi:10.2106/JBJS.G.01103.
- Kocher MS, Micheli LJ, Yaniv M, Zurakowski D, Ames A, Adrignolo AA. Functional and radiographic outcome of juvenile osteochondritis dissecans of the knee treated with transarticular arthroscopic drilling. Am J Sports Med. 2001;29(5):562-566. doi:10.1177/03635465010290050701.
- Adachi N, Deie M, Nakamae A, Ishikawa M, Motoyama M, Ochi M. Functional and radiographic outcome of stable juvenile osteochondritis dissecans of the knee treated with retroarticular drilling without bone grafting. Arthroscopy. 2009;25(2):145-152. doi:10.1016/j.arthro.2008.09.008.
- Kocher MS, Czarnecki JJ, Andersen JS, Micheli LJ. Internal fixation of juvenile osteochondritis dissecans lesions of the knee. Am J Sports Med. 2007;35(5):712-718. doi:10.1177/0363546506296608.
- Miura K, Ishibashi Y, Tsuda E, Sato H, Toh S. Results of arthroscopic fixation of osteochondritis dissecans lesion of the knee with cylindrical autogenous osteochondral plugs. Am J Sports Med. 2007;35(2):216-222. doi:10.1177/0363546506294360.
- Emmerson BC, Görtz S, Jamali AA, Chung C, Amiel D, Bugbee WD. Fresh osteochondral allografting in the treatment of osteochondritis dissecans of the femoral condyle. Am J Sports Med. 2007;35(6):907-914. doi:10.1177/0363546507299932.
- Gudas R, Simonaityte R, Cekanauskas E, Tamosiūnas R. A prospective, randomized clinical study of osteochondral autologous transplantation versus microfracture for the treatment of osteochondritis dissecans in the knee joint in children. J Pediatr Orthop. 2009;29(7):741-748. doi:10.1097/BPO.0b013e3181b8f6c7.

| Publication Date | 5/29/2014 |
| Article ID | 4 |
| Production ID | 0049 |
| Volume | 2014 |
| Issue | 4 |
| DOI | |
| https://doi.org/10.24296/jomi/4 | |